




![]()
![]()
![]()
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://ijmm.ir/article-1-1283-en.html



2- Department of Pulmonary Medicine, KVG Medical College, Sullia, India
3- Department of Microbiology, Lombard paramedical College and Allied Health Sciences and Hospital, Udupi, India
The coccidioides is a dimorphic fungus, that exist both in mycelia or as spherules. Both mycelia and spherules are asexual forms (1,2). The sexual form of coccidiosis has not been found. Two important species of this genus are C. immitis and C. occidioides posad-asii. The identification of the two species of coccidioi-des is difficult, only phenotypical methods are used. Therefore, in the routine diagnostic laboratory, cocci-dioides are not identified at the species level. The disease is also called as valley fever, which transmitted by inhalation of arthroconidia, the infectious particles of coccidiosis species, typically during periods of dry weather. The disease incubation period is usually between 10–16 days, which the majority of immune-competent patients who contract coccidioidomycosis will not develop any clinical symptoms or not seek medical attention (2-4). The infection usually prese-nts with non-specific respiratory and constitutional symptoms such as fever, cough, dyspnoea or fatigue. More severe complications of this infection are respiratory failure, severe sepsis, or disseminated coc-cidioidomycosis. Localised pneumonia, formation of pulmonary nodules (with or without cavitation), pleu-ral effusion or diffuse infiltrates are the severe compli-cations of the infection. The differential diagnosis of the infection if often difficult unless we have strong clinical and laboratory investigations (5,6). The main aim of the study is a reported case with coccidioido-mycosis to help in diagnosing the pulmonary infection.
A 57-year-old male, agriculturist by occupation from north Karnataka, presented to the Lombard memorial hospital with sudden loss of weight and appetite. He was a known case of IHD (Ischemic heart disease) with PIVD (Prolapsed intervertebral disc). After thorough physical and laboratory investigation found to have no abnormality, he was given appetite stimulant and sent home. After one month he came back with complaints of persistent weight loss of 8 kgs. His X-ray suggested left sided pleural infection, which was not present in his previous x-ray from our hospital (on the first visit). His Mantoux test and IGRA tests were positive for Tuberculosis. On clinical suspicion he was started empirically on anti-tuberculosis treatment (ATT) 2EHRZ + 4HER regimen although pleural fluid analysis was not conclusive. Even after two months of ATT, his chest X-ray showed persistent pleural infection (Fig. 1). His pleural fluid was aspirated and sent to microbe-ology and pathology laboratory. He developed dry cough, nausea, fever, deglutition difficulty. The patie-nt kept on losing weight. His laboratory findings revea-led predominantly lymphocytes (i.e1000 cells per cubic millimetre,cumm), sugar 63 milligrams per deci-litre (mgm/dL), protein 5.3 gram per decilitre (gm/dL) and adenosine deaminase (ADA) 105 Units per litre (U/L). Cartridge- based nucleic acid amplification test (CBNAAT) was negative for Tuberculosis. Bacteriology reports was sterile after 72 hours of incubation. Myco-logy culture report showed the colonies are moist, glabrous, membranous, and greyish initially, after 5 days of incubation white and cottony aerial mycelium was appeared (Figure 2). Further, the fungal wet mount preparation lactophenol cotton blue (LPCB) showed typical arthroconidiation with disjunctor cells (ghost cells) spherules suggest dimorphic fungi, C. immitis. The microscopically and cultural charact-eristics were also consistent with the C. immitis. After the mycology report, ATT regimen was stopped and started on azole drug (Itraconazole 200mg BID) for six weeks. After the antifungal treatment the patient’s chest X-ray was normal with no pleural infection. His appetite improved and he regained his weight.
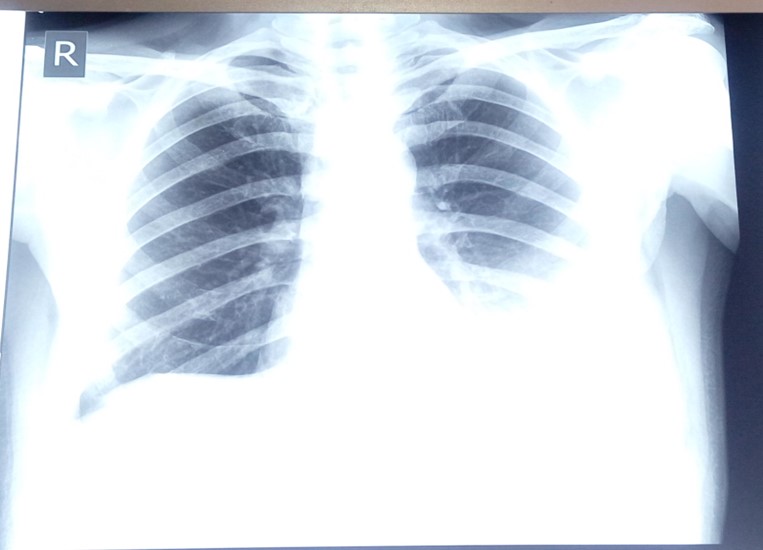
Figure 1. Chest X-ray showed Left sided pleural effusion at the presentation

Figure 2. Cultural characteristics: Sabouraud dextrose agar (SDA) showing gray whitish floccose, aerial mycelium.
The diagnosis of coccidioidomycosis, is often dela-yed. This is due to the less awareness of this condition while doing clinical diagnosis particularly in non-endemic regions (3). In the case of the patient in this study, the diagnosis was delayed because it was from a non-endemic region. This case made an impact on the clinical diagnosis and awareness. The pleural fluid analysis is actually not helpful, there is no diagnosis were made by analysis of this fluid, which may delay or exclude coccidioidomycosis (4,5,6). In the case the pleural infection, analysis was usual and there was no much impact on this infection. Coccidi-oidomycosis is usually mild disease in immunocomp-etent patients and often does not require antifungal therapy (7, 8). Other studies have shown that imm-uno-competent patients are produce rapid and more immune resp-onse to pulmonary coccidioidomycosis, leading to inc-reased pleural vascular permeability resulting in pleur-al infection formation. A fungal culture report will take time to report, this is the drawback of underdiagnosis of this disease (9,10).
The microbiological and pleural fluid analysis may not differ in both fungal and tuberculous pleural infection. A simple and routine mycological culture in all cases of pleural infection may help in the appr-opriate treatment and also for the diagnosis. Based on the radiological findings, it is always correlated with the microbiological culture, which may help in rule out the differential diagnosis.
We thank Dr Sushil Jathanna, Managing Director, CSI Lombard Memorial Hospital and Group of institutions, Udupi, for providing a facility for the study.
Conflicts of Interest
The authors declared no conflict of interest.
Received: 2021/02/23 | Accepted: 2021/07/10 | ePublished: 2021/08/16
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright Policy
Iranian Journal of Medical Microbiology by Farname is licensed under CC BY-NC 4.0![]()
![]()
![]()
