




![]()
![]()
![]()
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://ijmm.ir/article-1-1814-en.html

 , Payam Tabarsi2 , Mihan Pourabdollah Toutkaboni1 , Mehdi Kazempour Dizaji3 , Naghmeh Bahrami4 , Armita Narimani5 , Abdolreza Mohamadnia6 , Elham Askari1
, Payam Tabarsi2 , Mihan Pourabdollah Toutkaboni1 , Mehdi Kazempour Dizaji3 , Naghmeh Bahrami4 , Armita Narimani5 , Abdolreza Mohamadnia6 , Elham Askari1
2- Clinical Tuberculosis and Epidemiology Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran
3- Biostatistics Department, Mycobacteriology Research Center, National Research Institute of Tuberculosis and lung Diseases, Masih Daneshvari Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- Department of Tissue Engineering and Applied Cell Sciences, School of Advanced Technologies in Medicine, Tehran University of Medical Sciences, Tehran, Iran
5- Department of Cell and Molecular Biology, School of Biological Sciences, North Tehran Branch, Islamic Azad University, Tehran, Iran
6- Chronic Respiratory Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran ,
The Enterobacteriaceae family is the most heterogeneous group of clinically significant Gram-negative bacilli that are widely distributed in nature and can cause serious infections that lead to Nosocomial infection, also known as hospital infection or hospital-acquired infection (HAI), cystitis, pyelonephritis, pneumonia, meningitis, and more (1, 2). These bacteria are rod-shaped, nonspore-forming and are among the most important opportunistic pathogens, including many pathogens such as Klebsiella, Enterobacter, Citrobacter, Salmonella, Escherichia coli, Shigella, Proteus, Serratia and other species (3).
Pseudomonas is one of the genera of bacteria in this group. These Gram-negative bacteria are motile, aerobic, abundant in water and soil, and inhabit plants and animals (4). Pseudomonas sp. is present as normal flora on humans' skin, nostrils, and upper respiratory tract. It is also found in the intestines of more than 40% of healthy people. This percentage increases in hospitalized patients relative to the average length of hospital stay (5). The most important species of this genus is Pseudomonas aeruginosa, which can cause infections in the blood, lungs (pneumonia), or other body parts after surgery in patients with autoimmune disease (6). This bacterium is the third leading cause of nosocomial infections after Staphylococcus aureus and Escherichia coli, and it is in the "critical group" list of the WHO (7). P. aeruginosa has native resistance to penicillin and most beta-lactam antibiotics (8). Acinetobacter baumannii, another Gram-negative bacterium, is an opportunistic pathogen that mainly causes nosocomial infections, particularly in patients admitted to the intensive care unit (ICU) (9). This bacterium contributes to infections such as UTI, pneumonia, and sepsis during and after hospitalization (10). Recent reports have indicated resistance to carbapenems and cephalosporins among Enterobacteriaceae (11, 12).
Resistance mechanisms to antimicrobial agents can be intrinsic and acquired. The latter mechanisms result from mutational events (especially for quinolone resistance) or, more often, the acquisition of various mobile genetic elements such as transposons and plasmids. First reported in the early 1980s in Germany and France, a major problem in the medical field in recent times is the increasing number of Enterobacteriaceae strains found to produce extended-spectrum β-lactamases (ESBLs) (13, 14).
Beta-lactams, especially broad-spectrum cephalosporins and fluoroquinolones, are the first-line treatment for infections caused by Gram-negative bacteria (15, 16). However, one of the major challenges associated with treating these bacterial infections is the Emergence of multi-drug resistant (MDR) isolates, which can be possibly due to the widespread and uncontrolled use of antimicrobial agents, especially in developing countries (16). Developed in the 1980s, carbapenems (the most widely used is imipenem, followed by meropenem and ertapenem) are derivatives of thienamycin and have broad-spectrum activities and are used to treat infections caused by ESBL-producing strains.
Among beta-lactamase enzymes, Carbapenemases and Metallo-beta-lactamases are the most important, causing major problems in treating infectious diseases due to their effect on a wide range of antibiotics such as penicillin, broad-spectrum cephalosporins, and carbapenems (17-19). Therefore, it is crucial to study the presence and frequency of these enzymes in clinical isolates to control the spread of antibiotic-resistant bacteria and detect infections caused by these pathogens at an early stage.
The present study aimed to identify carbapenemase-producing strains of Gram-negative isolated bacteria and determine their antibiotic susceptibility pattern in samples obtained from the Masih Daneshvari hospital, Tehran, Iran.
Sample Collection
This cross-sectional study was conducted from March 2021 to March 2022 in Masih Daneshvari Hospital, Iran. 1600 samples were collected randomly from the Clinical Laboratory of Masih Daneshvari hospital, Tehran, Iran, from various clinical specimens, including urine, respiratory tract, abdominal fluid, and blood. For this purpose, all incoming samples were checked, suspicious or weak samples were excluded from the study, and the samples confirmed in the bacteriology department were included. These samples were then examined for isolation of Gram-negative bacteria. To identify these bacteria, samples were cultured on MacConkey agar. Gram-negative bacilli were then inoculated into different media, including Simmons Citrate agar, Kligler's Iron agar, Methyl Red / Voges-Proskauer and Triple Sugar Iron agar (Neogen, Italy). After 24 hours of incubation at 37°C, the colonies were isolated. Subsequently, oxidase and urease tests were performed for the isolated bacteria.
Antibiotic Susceptibility Test
Antibiotic susceptibility test for bacterial strains was determined by the Kirby-Bauer disk diffusion method on Mueller-Hinton agar, according to the recommendation of the Clinical and Laboratory Standards Institute (CLSI, 2020), using imipenem (10 μg/mL) and meropenem (10 μg/mL).
For this purpose, we initially prepared a Mueller-Hinton agar and a bacterial suspension with turbidity equivalent to 0.5 McFarland. Then, the suspension was cultured on the Mueller-Hinton agar by swabbing a sterile swab in three different directions. After 15 minutes of complete application of the microbial suspension on the medium, the antibiotic discs were placed 2 cm apart. Finally, after 24 hours of incubation at 37 °C, the diameter of the grown halos was measured by a ruler and assessed based on the CLSI instructions (13).
Quality control strains of Escherichia coli ATCC®* 25922 and Pseudomonas aeruginosa ATCC® 27853 (for carbapenems) were used to validate the results of the antimicrobial discs.
Evolution of Carbapenemase-encoding Genes
Also, the real-time polymerase chain reaction (Real-time PCR) method was used for the molecular evaluation of carbapenemase-encoding genes. For this purpose, 250 samples were randomly selected. Then, several bacteria colonies were cultured in 10 mL of Tryptic Soy Broth (TSB) medium. After 24 hours of incubation at 37-35 °C, DNA extraction was performed using a DNA extraction kit (Yekta-tajhiz Co., Iran). Real-time PCR in 2 biological replicates was performed using a real-time PCR system (Applied Biosystems StepOne instrument), SYBR Green Master Mix and sets of primers (Table 1). The StepOne software (Applied Biosystems; version 2.1) was used to analyze the results (19-25).
Table 1. Primer sequences used for gene expression analysis by quantitative PCR (26)
| Genes | Sequence (5' à 3') | Annealing temperature | Amplicon length (bp) |
| oxa -48 | F: TGGTGGCATCGATTATCG R: AGCACTTCTTTTGTGATG |
58˚C | 743 |
| kpc | F: TCGAACAGGACTTTGGC R: GAACCAGCGCATTTTTG |
57˚C | 489 |
| ndm | F: CCGCCTGGACCGATGACC R: CCAAAGTTGGGCGCGGT |
60˚C | 263 |
| imp | F: AGGCGTTTATGTTCATAC R: GTAAGTTTCAAGAGTGAT |
53˚C | 585 |
| vim | F: TTGGTCGCATATCGCAAC R: AATGCGCAGCACCAGGAT |
58˚C | 261 |
| ges | F: GCGCTTCATTCACGCAC R: CTATTTGTCCGTGCTCAG |
57˚C | 640 |
| β-globulin (housekeeping) | F: AGAGTTTGATCCTGGCTCAG R: GGTTACCTTGTTACGACTT |
55˚C | 120 |
Carrying out the Real-time RT-PCR test by HotTaq EvaGreen qPCR Mix:
SYBR Green is a fluorescence color that has been used in the kit produced by Cynacolon Company (Cat No.BT11101, Iran). The components needed for reaction have been provided in mastermix of the kit. The components of Real-time PCR reaction included the following cases: Extracted DNA 2 μL (50 ng/μL), Master mix at 4 μL, Primer forward and reverse 10 pmol, Deionized distilled water to an extent in which the final reaction volume reaches 20 μL
The temperatures and reaction program was adjusted according to the kit's instructions (Table 2).
Statistical Analysis
Susceptibility data were compared by using a Chi-square test with SPSS (SPSS Inc., Chicago, Ill. USA) version 20 software. We calculated susceptibility and resistance as percentages based on a 95% confidence interval. Based on the categories of the selected variable, cross-tabulations of the presence of resistant/intermediate/susceptible isolates were performed. Statistical significance was defined as a P value of 0.05.
Table 2. Real-time RT-PCR reaction temperatures and times
| Real-time step | Temperature | Duration |
| Initial activation | 95ºC | 10 min |
| 40 cycles | ||
| Denaturation | 59ºC | 15 Sec |
| Annealing | 56-60ºC | 60 Sec |
| Extension | 72ºC | 20 Sec |
While the most frequently isolated bacteria was Pseudomonas aeruginosa (37.3%), the lowest frequency was for Enterococci (0.4%). The frequency of bacterial strain isolates is shown in Figure 1.

Figure1. The frequency of isolates in terms of bacterial strain
200 (80%) of 250 tested isolates had resistance genes to at least one antibiotic resistance gene. The following carbapenemase genes were most frequently detected among carbapenem-resistant strains: imp (70 isolates; 35%), vim (40 isolates; 20%), kpc (30 isolates; 15%), oxa -48 (20 isolates; 10%), ndm (20 isolates; 10%), and GES (20 isolate; 10%).
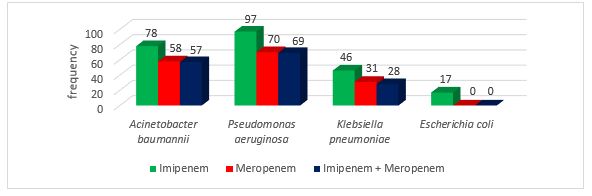
Figure 2. The frequency of resistance in carbapenem-resistant Gram-negative bacilli
Although antibiotic resistance in bacteria isolated from hospitalized patients, as well as bacteria with a direct detrimental effect on human health, has been a research focus in recent years, it is important to know that the development of resistance to antibiotics is a natural ecological phenomenon (26). In response to the Emergence of microbial resistance to various antibiotics, a large number of antibiotics have been produced and introduced over the past two decades (27). Nevertheless, the growing trend of resistance to certain antibiotics on the one hand, and the identification of potentially modifiable factors contributing to microbial resistance, on the other hand, have posed great challenges for physicians (28).
In recent years, there have been many reports of Enterobacteriaceae strains producing carbapenemase enzymes worldwide. Although these enzymes are often found in Klebsiella pneumoniae, there are reports of these enzymes found in other bacteria of this large family, including Enterobacter, Salmonella, and Escherichia coli (28, 29).
There are three main mechanisms by which Gram-negative bacteria resist carbapenems. These include enzymatic hydrolysis of carbapenems by Carbapenemases that are encoded by the following genes: ndm, kpc, ampC , vim, oxa, and imp; expression of efflux pumps that actively remove carbapenems from the bacterial cell; and reducing the permeability of bacterial outer membrane through porin loss along with overexpression of ampC and esbl beta-lactamases (29-31).
In a report by Shahcheraghi et al. that studied Enterobacteriaceae isolated from hospitals in Tehran, 3.6% of the samples were resistant to meropenem, 0.3% were resistant to ertapenem, and 1.1% were resistant to imipenem (32). Solgi et al. found that 88% of Enterobacteriaceae, Pseudomonas aeruginosa, and Acinetobacter baumannii strains were resistant to imipenem and meropenem, indicating an increase in bacterial resistance to carbapenems in recent years (33). Also, in the study by Solgi et al., of a total of 44 Gram-negative strains that were resistant to antibiotics, 17 were positive for Carbapenemases. Among these, only four had the imp gene, while none of the other genes (oxa -48, vim, ges, ndm, spm and kpc) were detected in any isolates (33). Kumarasamy and colleagues showed that the prevalence of beta-lactamases (ndm1, vim, and imp) among multidrug-resistant Enterobacteriaceae varies between 31% and 55% (34).
The incidence and prevalence of carbapenem-susceptible Enterobacteriaceae (CSE) could be influenced by geographical factors (35, 36). According to reports from Mexico and Uganda, the prevalence of CSE is about 10%. While CSE rates are reported to be approximately 0.6% in Asia, this rate is 2.93 percent per 100,000 people in the United States (37, 38). Patients with severe illnesses, such as those undergoing mechanical ventilation, intensive care, and transplantation, or those hospitalized for a long time and have had long-term antibiotic use, are at risk for carbapenem-resistant Enterobacteriaceae (CRE) infections (39, 40).
Differences in the mention results may be due to variation in clinical samples, study time, and treatment strategies in each geographic area. However, all studies indicate that resistance to most antibiotics has increased in Gram-negative bacteria, including Pseudomonas and Acinetobacter. This could be due to the continuous and inaccurate use of antibiotics in long-term hospitalizations as well as the lack of proper infection control measures in hospitals.
The present study shows that the rate of drug resistance as well as the production of beta-lactamase enzymes in gram-negative strains such as Enterobacteriaceae, Pseudomonas and Acinetobacter is high and therefore the treatment of infections caused by these bacteria may be difficult. Therefore, early detection of carbapenemase-producing bacteria will be important to reduce mortality and the prevalence of multidrug-resistant organisms. In addition, by using the correct pattern of antibiotic use and limiting the use of beta-lactam drugs, especially broad-spectrum cephalosporins, and by using rotational programs of antibiotics, it is hoped that the prevalence of carbapenemase-producing strains and other patterns of drug resistance in different parts of the hospital.
All procedures were approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (Ethics code: IR.SBMU.MSP.REC.1398.287). All patient information were kept confidential during all stages of the study.
This research is a part of the efforts of the professors and colleagues of Masih Daneshvari Hospital of Shahid Beheshti University of Medical Sciences. All involved are sincerely thanked.
Conflicts of Interest
There is no conflict of interest between the authors.
None.
Received: 2022/07/7 | Accepted: 2022/08/18 | ePublished: 2022/09/9
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright Policy
Iranian Journal of Medical Microbiology by Farname is licensed under CC BY-NC 4.0![]()
![]()
![]()
