




![]()
![]()
![]()
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://ijmm.ir/article-1-1046-en.html



2- Student Research Committee, Kurdistan University of Medical Sciences, Sanandaj, Iran.
A fter cardiovascular diseases, cancer is the second agent of the worldwide death and the third agent in Iran after driving accidents and cardiovascular diseases (1). Based on the last estimate of world health organization, cancer is the cause for death of 13% of world’s population annually (1). 70% of cancer-related deaths occur in developing countries such as Iran (2). In this regard, gastric cancer leads to 8,000 deaths in Iran annually (3). The prevalence of cancers in different areas of Iran is not the same (3). Sanandaj city as Kurdistan province center in west of Iran, has high prevalence of gastric cancer patients (4-6). Kurdish people in Sanandaj city have some differences in economic conditions, diet and other customs than other big cities in Iran (4). In the previous studies, Helicobacter pylori infection, age, sex, economic and educational situation of patients have been considered as interferer risk factors on the prevalence of gastric cancer (6-10). In this study, the statistical relation of H. pylori infection and demographic variables such as age, sex, occupation and education levels have been surveyed in gastritis and gastric adenocarcinoma patients referred to Tohid and Shaheed Ghazi hospitals in Sanandaj city during October 2017 to March 2018.
In an analytical cross-sectional study, the demographic factors of gastritis and gastric cancer patients including sex, age, education and occupation and active H. pylori infection were analyzed. Patients were included by consecutive and convenience sampling method. All patients had referred to Tohid and Shaheed Ghazi hospitals in Sanandaj city during 18 months from September 2017 to March 2018. Gastritis and gastric cancer patients under antibacterial chemotherapy were excluded. Clinical symptoms of gastritis and gastric cancer were diagnosed by gastroenterologist using endoscopy. The number of cases was calculated according to the prevalence of gastric cancer in Sanandaj city with a confidence level of 0.05 and 95% confidence interval using Cochran formula. A total of 50 gastritis patients as the control group and 50 gastric adenocarcinoma patients as the target group were selected. Patients with positive urease breath test were considered as H. pylori active infection. Patients' demographic information was obtained by direct questions from patient or patient’s companion. Histopathology data of each gastric adenocarcinoma patient was collected from the records in hospitals. TNM classification is one of the recommended methods for staging of gastric adenocarcinoma (11). This procedure determines the size and progression of tumor mass (T), the number of lymph nodes involved in adjacent of tumor areas (N) and the spread of tumor cells to other tissues or metastasis (M) (12). Another system of cancer detection is the Numerical system, which is reported in gastric cancer as G0, G1, G2, G3 and G4 (12). In this system, G0 is reported when cells of tumor mass are poorly differentiated to normal cells and cancer cells are not proliferated (12). At the other end of this categorization system, G4 is reported when cancer cells are good differentiated to normal cells and have spread to other tissues or have been metastasized (12). Tumor staging of gastric adenocarcinoma tumor in this study was recorded based on Number system. Data statistical analysis was performed for sex, age, occupation and education situation and H. pylori infection related to clinical results of patients including gastritis, gastric cancer, adenocarcinoma anatomic areas and tumor grades by SPSS 25 (SPSS Inc., Chicago, Ill., USA) using Chi-square, Fisher exact tests and descriptive statistics.
Data analysis showed that the highest percentage of thA total of 64 male and 36 female subjects were included in this study. In the male group, 24 (37.5%) and 40 (62.5%) patients had gastritis and gastric cancer respectively. In the female group, 26 (72.22%) and 10 (27.88%) patients had gastritis and gastric cancer respectively. The results of Chi-square tests showed there is a significant relationship between sex and disease (P=0.001), because the prevalence of gastric cancer was four times higher in male subjects (Table 1). As expected, like Others’ studies most cases of gastric cancer were in the age group of 76-85 years old (36%) and the lowest rate was in the age group of 18-30 years old (0%) (Figure 1). The highest and lowest prevalence of gastritis were in 31-45 (36%) and 76-85 (0%) years old respectively. 47% of all patients had H. pylori active infection that 24 and 23 cases were gastric cancer and gastritis respectively. Among patients without H. pylori active infection, 26 (49.1%) and 27 (50.9%) cases had gastric cancer and gastritis respectively. H. pylori infection did not statically show any significant relation with the prevalence of gastric cancer (P=0.841). In terms of age, as it increased, in the female population, the prevalence of gastric cancer and gastritis increased. In the male population, 40 (62.5%) and 24 (37.5%) cases had gastric cancer and gastritis respectively. In the female population, 10 (28.8%) and 26 (72.2%) cases had gastric cancer and gastritis respectively. The correlation between sex and age of patients with gastric cancer was statistically significant (P=0.001 and P=0.000 respectively) (Table 1). Figure 1 expresses the frequency of gastritis that decreases as the age increases and the frequency of gastric cancer that increases as the factor age increases (Spearman correlation coefficient= 0.764). Figure 2 shows the prevalence of gastritis and gastric cancer in the occupational groups. In the 100 patients studied, 54 were workless, 27 were self-employed and 19 were government employees. Spearman correlation test showed there was a weak inverse correlation between occupation situation and disease (Spearman correlation coefficient= -0.187). The results of Chi-square test showed a statistically significant relationship between age and occupation with gastric cancer (P=0.061 and P=0.070 respectively) and H. pylori infection with tumor grade (P=0.082) (Table 1). However, to consider the type I error significance level was set to 0.05, the results of correlations higher than 0.05 were not considered as statistically significant (P> 0.05). Figure 3 shows prevalence of gastritis and gastric cancer in educational groups. As we expected the higher prevalence of gastric cancer was in patients without education and showed a statistically strong significant relationship (P=0.000). The correlation between gastritis and the three degrees of education was not statistically significant. The results of this study showed that the prevalence of gastric cancer decreases with increasing of education level (Spearman correlation coefficient -0.484). The prevalence of gastric cancer tumor areas in the 50 gastric adenocarcinoma patients were 20, 8, 8 and 14 cases for cardia, gastric body, lesion curvature and antrum respectively. The frequency of G1, G2, G3 and G4 tumor grades in 50 gastric adenocarcinoma patients were 11, 22, 13 and 4 respectively. There was not any statistical correlation between tumor grades and anatomic region of gastric carcinoma (Spearman correlation coefficient = -0.047). The results of study showed there is a direct but weak correlation between H. pylori infection and anatomic areas of gastric adenocarcinoma (Spearman's coefficient = 0.356). Most of patients with gastric adenocarcinoma in cardia area had H. pylori active infection that did not show a statistically significant relationship using Chi-square test (Table 1).
Table 1. Statical Survey of quality data was performed by SPSS 25 using χ2 test. The results of χ2 test showed a significance relationship between kind of disease and sexuality, age and education level (P< 0.05).
| Variable | Disease | Tumor area | Tumor grade | |||
| χ2 | P-value | χ2 | P-value | χ2 | P-value | |
| H. pylori infection | 0.040 | 0.841 | 6.702 | 0.082 | 4.673 | 0.548 |
| Sexuality | 11.111 | 0.001 | 3.237 | 0.357 | 0.361 | 0.948 |
| Age group | 40.144 | 0.000 | 9.477 | 0.394 | 16.310 | 0.061 |
| Occupation | 5.333 | 0.069 | 13.898 | 0.126 | 15.842 | 0.070 |
| Education | 23.667 | 0.000 | 8.257 | 0.220 | 4.673 | 0.586 |
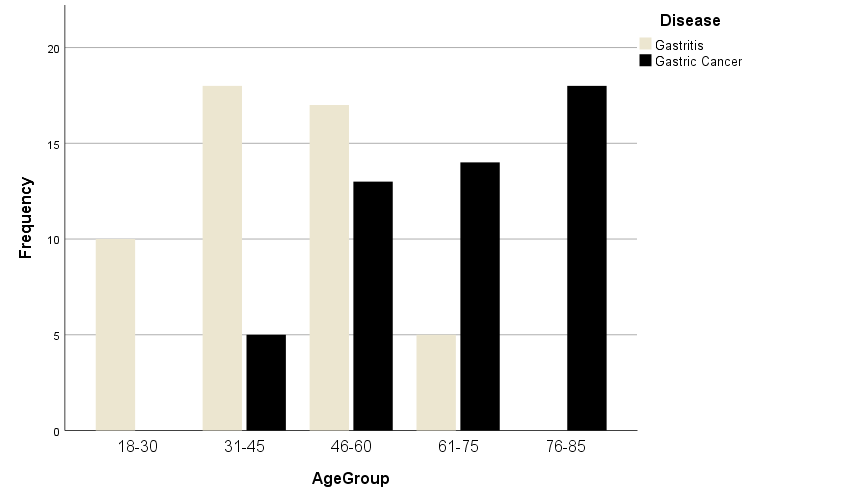
Figure 1. Clustered bar of frequency of five age groups in gastritis and gastric cancer patients.

Figure 2. Clustered bar of frequency of three occupation situations in gastritis and gastric cancer patients.

Figure 3. Clustered bar of frequency of five education levels in gastritis and gastric cancer patients.

Figure 4. Prevalence map of gastric cancer in 30 provinces of Iran in 2014.
The previous studies showed the highest prevalence of gastric cancer in the geographical areas of northwest, north and west in Iran, respectively. 50% of gastric cancers have occurred in Gilan province, a northern province in Iran (2). All previous data show that Ardabil, Zanjan, and Azerbaijan provinces have a high incidence of gastric cancer, more than 30 cases per 100,000 people. Ilam and Kurdistan provinces have 20-30 cases per 100,000 people (Figure 4). Some studies have shown the high prevalence of gastric cancer in some areas of Iran due to specific diets such as high-fat, high-salt and custom habits such as dinking hot tea and tobacco consumption (1-2). The highest and lowest rate of gastric cancer in Iranian people are in the age group of 75 to 85 and 60 to 64 years old respectively. Overall, the prevalence of the most common cancers in Iran is included breast cancer 2%, prostate cancer 2%, skin cancer 2%, gastric cancer 2% and colon cancer 5% (2). Based on the study performed in Iran in 2014, 54% of all cancers were observed in men and the most common kind of cancer were gastric cancer and breast cancer in men and women respectively (2). The most common cancers in Kurdistan province are included skin, stomach, breast, esophageal, colorectal and bladder cancer with frequency of 285, 221, 128, 121, 109 and 100 cases per 100,000 people respectively (2).
Although H. pylori active infection could lead to chronic gastritis, 85% of people with H. pylori active infection do not complain during their lives (14). In some infectious people, gastric chronic inflammation could progress to peptic ulcer and gastric cancer (15-16). In developed countries, the prevalence of H. pylori infection increases from 10% at childhood age to 50% or less at the age of 50 (17). The prevalence of H. pylori infection in Iran is also high, with a prevalence of up to 69% (17). Other studies have shown that prevalence of H. pylori infection is 35-50% in Sanandaj city (20).
The results of our study showed that prevalence of H. pylori infection is 47% of gastric (23 of 50) and gastric cancer (24 of 50) patients. The highest and lowest prevalence of H. pylori infection were in the age groups of 45-60 and 18-30 years old with 15 and 2 patients respectively. The prevalence of H. pylori infection in female and male patients was 17 of 36 and 30 of 64 respectively. Totally, the results of this study about the prevalence of H. pylori infection was in line with other studies.
The risk of cancer increases as people become older (21-22). Most cases of cancer occur in people over 55 years old with the mean age of 70 years in men and 74 years in women (1-2). However, some kinds of cancers, such as the blood and the nervous system cancers are more prevalent at younger ages even below 15 years old (1-2). The results of this study showed an increase in the incidence of gastric cancer as patients’ age increased.
The prevalence of most common cancers in women is lower than men (1, 2, 23). It is estimated up to 2 times for men (2). Sexuality is an important factor in the epidemiology of cancers. Regarding the incidence risk of gastric cancer, men are 2 times more in danger than women (5-7). According to the newest data from the National Cancer Research Center, gastric cancer is the most common kind of cancer in men and the third most common kind of cancer in women after breast and colon cancers respectively worldwide (2). Accordingly, the ratio of men to women is 2.9 times which in most cases occur at poor and lower socioeconomic levels (2). The ratio of incidence of gastric cancer in men comparing to women is 1.54 in the USA. This ratio for some cities in Iran such as Shiraz, Tehran and Ardabil is 2.2, 3.3 and 2.33 respectively (1, 2). The results of our study showed that out of 50 gastric adenocarcinomas just 10 patients were female and the ratio of incidence of gastric cancer in men was 4 times compared to women. The results of our study maybe had been due to the cultural and traditional behaviors in women; showing high rates in male subjects due to be exposed to occupational risk factors in Kurdistan province.
A dozen of social variables such as occupation and education are involved in the situation of society health (7-9, 23-24). The kind of job and level of education effect the life quality directly (7-9). Another study showed that over 70% of Kurdistan people are without educations (25). The capita of students in Iran is 4760 per 100,000 population while in Kurdistan province is 2691 and lower than country average (25). Jobs as the sources of income have a direct impact on people's lifestyle. In general, poor and low-income populations are at the exposure of risk factors (5-6). On the other side some studies have shown that some jobs such as radiologists are at more risky of cancer incidence (19-20 and 22). Focus on mental effects tell us that people with stable income are less exposed to stress and incidence of cancers (8-10). The results of our study showed that the incidence of gastric cancer decreases as increasing mental quality of job and education level in population. In this regard, the lowest and highest prevalence of gastric cancer are in the government occupational group with a stable incoming and workless group with no income. The prevalence of gastric cancer was inversely correlated with the level of education. In this regards, the lowest prevalence of gastric cancer was observed in the postgraduate alumni group.
A study by Hur et al. (2012) showed upper gastric area or cardia has a different pathological and epidemiological characters from adenocarcinoma tumors in other areas of the stomach. Although cardia tumor occurs in non-colonized H. pylori area but is associated with H. pylori infection (14). Hur et al. showed that H. pylori infection is associated with G3 and G4 of gastric adenocarcinoma tumor stage (P= 0.019) (14). In our study, the greatest number of H. pylori infection was observed in gastric cancer patients at cardia area. Although cardia area with 20 cases, it was the predominant tumor area in gastric adenocarcinoma patients but no significant correlation was found between H. pylori infection and cardia tumor area. There was a statistical relationship between age and occupational groups with the tumor grades close to error level 0.05 (P=0.061 and P=0.070 respectively).
Overall, the results of our study showed that the impact of social factors on prevalence of gastric cancer in Kurdistan province is similar to the pattern of the other developing countries with high incidence. Although the genetic risk factors should not be waived at incidence of gastric adenocarcinoma.
The present study which has been funded by Kurdistan University of Medical Sciences, is student dissertation of Ms. Delniya Khani with accompaniment of Dr. Manouchehr Ahmadi Hedayati as supervisor. Ethics Codes are IR.MUK.REC.1397/82 and IR.MUK.REC.1397/195. Thanks to Dr. Roghayeh Ghadyani and Dr. Farshad Sheikhesmaeili for sampling support.
Authors declared no conflict of interests.
Received: 2020/01/19 | Accepted: 2020/02/5 | ePublished: 2020/03/14
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright Policy
Iranian Journal of Medical Microbiology by Farname is licensed under CC BY-NC 4.0![]()
![]()
![]()
